C-sections – On The Rise
Rising rates
C-section rates have been rising in the UK and in other high- and middle-income countries. The UK has some of the highest, and fastest rising rates in Europe. In Scotland 38% of all births in 2021 were by C-section (1) closely followed by England (35%), Northern Ireland (34%) and Wales (31%). Yet the World Health Organisation suggests C-section rates above 15% are unlikely to improve maternal and neonatal health (2) while their overuse can also be a drain on human and financial resources.
Why? We don’t know for sure, but a range of factors - from maternal age to obesity - may be involved. It could also be that increasing risk aversion on the part of medical staff and management, coupled with a growing blame culture and fear of litigation, is driving the increase (1).
Women’s beliefs about the relative safety of surgery may also be a factor, and women may be making more requests for C-sections. The National Institute for Clinical Excellence (NICE) does support women who request C-sections, but Health Trusts and Boards differ in the way this guidance is implemented.
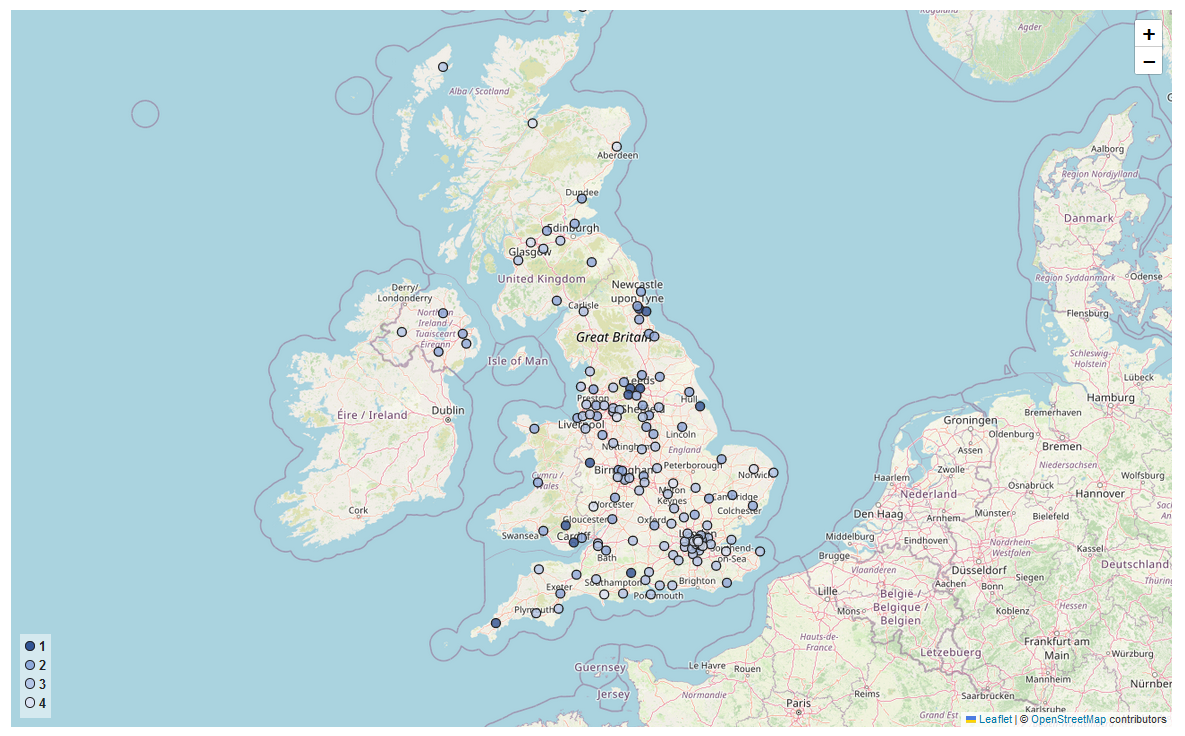
What is clear however, is that socio-economic status and ethnicity are important factors in C-section rates. Women who live in better off areas have more C-sections, as do women from Black and Asian backgrounds. And marked differences are seen between trusts (see map).
C-section by ethnicity
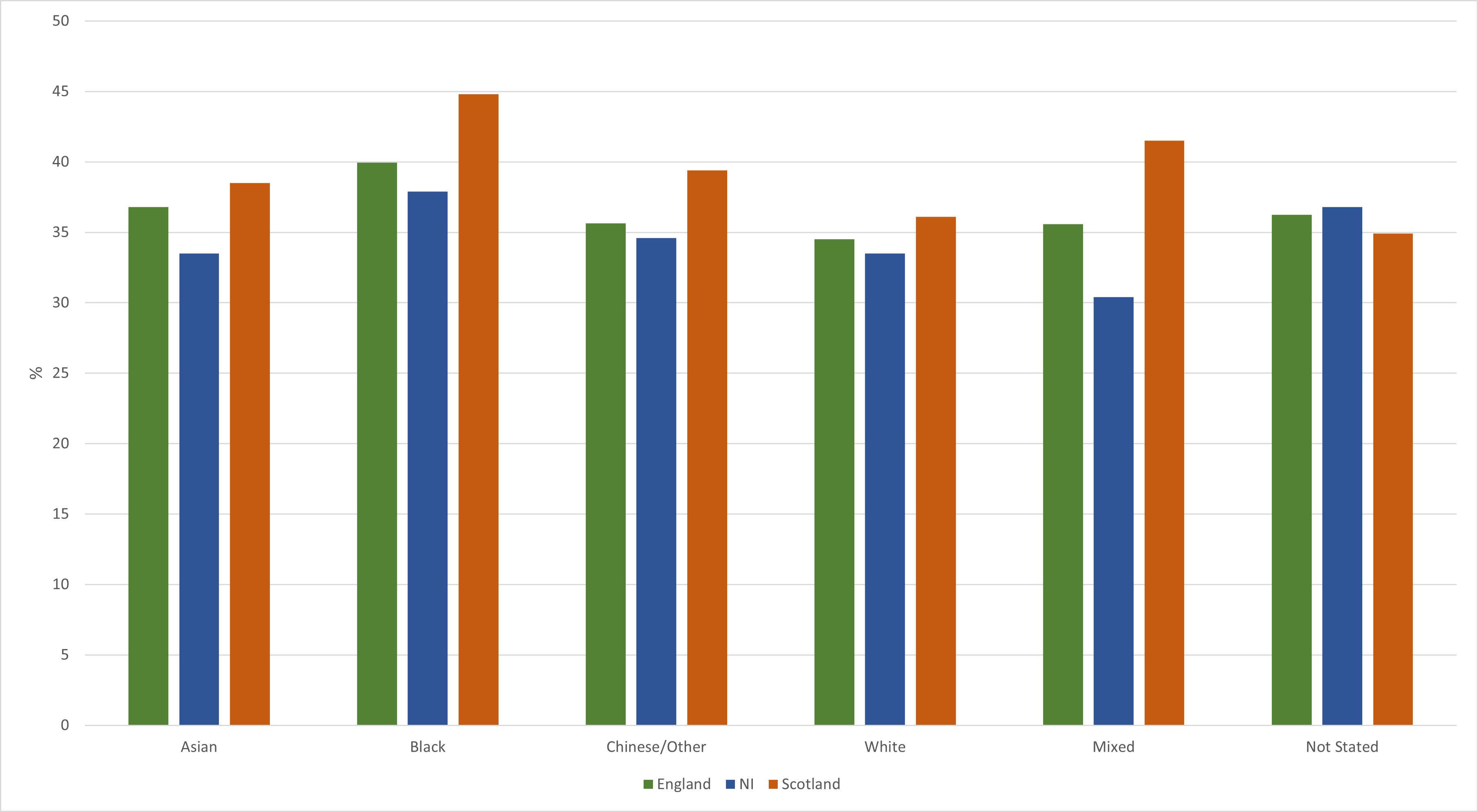
Note: data for England from 2021/22, NI from 2020/21, Scotland from 2021, Wales from 2021. See map for details of data sources for each nation.
Risks for the mother, risks for the baby
C-sections can be lifesaving for both mother and child. Yet, as with any surgery, they involve risks. When there is no medical or obstetric indication for the operation it is especially important to consider the risks of C-sections versus any potential benefits. (3)
C-section can mean a longer hospital stay for the mother. It can also increase the risk of hysterectomy and of a ruptured uterus in future pregnancies. For babies, C-sections can also increase the risk of neonatal unit admissions and of longer-term disorders such as asthma, and of childhood obesity (4). NICE does not report any benefits for babies following C-section in women with no complications (3).
 Click here to view the C-section data
Click here to view the C-section dataResponding to rising rates
All women have the right to safe and personalised maternity care which gives them choice and control over their own options. However, in response to the population level harms of rapidly rising rates, various countries have taken initiatives to reduce C-sections when there are no medical or severe psychological reasons for them.
In California, a state-wide programme from 2015 to 2020 aimed to lower C-section rates for low-risk women. The programme monitored data, created toolkits for care providers and promoted patient engagement. Within four years the rates were reduced. (5)
Other factors can also reduce C-section rates. Good quality, supportive midwifery-led care, with continuity of care can increase rates of spontaneous birth. Continuous support in labour, out-of-hospital birth, and use of intermittent rather than continuous fetal monitoring are all associated with lower rates of C-section, with no change in fetal mortality or morbidity. (6)
Any drive to reduce C-section rates must ensure that women who need and want to give birth by C-section can do so. But women have a right to accurate information about the risks and advantages. Midwives and other health providers should listen to women who want a C-section and discuss the risks and benefits in a way that is understandable and accessible.
Whatever their choice, women must be offered skilled, compassionate, and equitable care during labour and birth.
Reference links
- Caesarean Section Rates. 2021 [cited 2023 Jun 12]; Available from: http://www.gov.scot/publications/best-start-review-caesarean-section-rates-scotland/pages/3/
- http://www.thelancet.com/article/S0140673618323948/fulltext
- www.nice.org.uk/guidance/ng192
- Long-term risks and benefits associated with cesarean delivery for mother, baby, and subsequent pregnancies: Systematic review and meta-analysis - PubMed (nih.gov)
- https://www.chcf.org/project/reducing-unnecessary-c-sections/#related-links-and-downloads
- Midwife-led continuity models versus other models of care for childbearing women - PubMed (nih.gov)